|
LA MUMMIA DI TORRICELLA PELIGNA
di Prof. Luigi Capasso, Il rinvenimento di un corpo mummificato nei sotteranei della chiesa di San Giacomo Apostolo a Torricella Peligna è un evento di notevole interesse storico e scientifico, che ha fornito un'occasione di studio per quanto riguarda le caratteristiche di questo reperto, soprattutto relativamente al suo inquadramento storico-sociale, antropologico e medico- scientifico.
La
mummia di Torricella Peligna è ben conservata, ma il suo
ritrovamento e la
L'intervento di restauro prevede l'eliminazione (tramite disinfettanti gassosi immessi attraverso complicate manovre) di tutti gli agenti distruttori, dai più minuti (batteri), a quelli macroscopici (insetti). La successiva conservazione è basata sulla realizzazione di un "microclima confinato", cioè di una teca con atmosfera di azoto, incompatibile con qualsiasi forma di vita, isolata dall'ambiente esterno RELAZIONE ANTROPOLOGICA Inquadramento Medico-Scientifico La mummificazione è un evento eccezionale, in quanto dopo la morte il cadavere generalmente subisce una decomposizione che porta alla scheletrificazione. Il processo di mummificazione dei tessuti molli si può verificare sia per processi naturali che per manipolazioni artificiali. La mummificazione artificiale è quella che veniva praticata nell'antico Egitto e che ha conservato fino ai giorni nostri una notevole quantità di reperti, ancora oggi oggetto di studi in tutto il mondo. La mummificazione naturale si verifica con modalità diverse (saponificazione, mummificazione in torba, mummificazione spontanea), la più nota e diffusa delle quali è la mummificazione spontanea. Il processo di mummificazione spontanea si verifica in condizioni climatiche ben precise e cioè quando l'ambiente di inumazione è molto secco e arieggiato. Questo fatto comporta la rapida disidratazione dei tessuti molli e, quindi, blocca l'azione degli enzimi tissutali responsabili dei processi di autolisi. Altra condizione in grado di influenzare il processo di mummificazione spontanea è lo stato di nutrizione del soggetto al momento del decesso, essendo più facile e rapida la mummificazione di soggetti cachettici. Descrizione del reperto La mummia in oggetto rappresenta un corpo disteso in posizione supina, con arti superiori ed inferiori estesi, il cui stato di conservazione è globalmente discreto pur essendo molto diverso da un punto del corpo all'altro. La testa si presenta disarticolata dal corpo e mostra alcune parti della volta che sono prive di cute, inoltre manca il padiglione auricolare destro. Il tronco è in buono stato di conservazione e non presenta soluzioni di continuità della cute, mentre negli arti superiori e inferiori sono visibili, in alcuni punti, parti dello scheletro osseo. Sono visibili, un po' ovunque, resti di insetti morti che hanno lasciato segni evidenti della loro opera di demolizione. Descrizione antropologica Il corpo mummificato é quello di un soggetto di sesso maschile e di età adulta. I caratteri sessuali secondari tipici del sesso maschile, espressi a livello del cranio, sono rappresentati dalla generale robustezza dei punti di inserzione dei muscoli masticatori, nucali e della fronte, dalla morfologia della mandibola, più squadrata e "forte" nel sesso maschile, e da una maggiore robustezza dei vari segmenti ossei in generale. Nel nostro soggetto questi caratteri sono stati valutati sia all'osservazione diretta che su radiogramma e si evidenziano come una forte espressione dell'arco sopraciliare, della glabella, dei rilievi del piano nucale e del processo zigomatico del temporale; inoltre il corpo della mandibola è piuttosto grosso, presenta un mento prominente, acuto di profilo, con doppia protuberanza mentale, mentre il suo gonion esprime un processo lemuroide molto marcato, punto di inserzione di un muscolo massetere molto potente. A livello del bacino sono stati rinvenuti organi genitali esterni di tipo maschile cui corrispondono caratteristiche antropologiche del bacino osseo di tipo androide, con le ali dell'ileo piuttosto strette e verticali ed una incisura ischiatica stretta.
Per quanto riguarda la determinazione dell'età al
momento della morte é stato La statura in vita, misurata direttamente sul corpo mummificato, è di circa 164 centimetri. Datazione della sepoltura Allo scopo di stabilire l'epoca della sepoltura, sono stati prelevati tre campioni di materiale organico, provenienti dalla sepoltura stessa, che sono stati sottoposti ad analisi di cronologia radiometrica con il metodo del radiocarbonio. I materiali esaminati erano rappresentati da: 1) frammenti di paglia provenienti dal cuscino della salma; 2) frammenti di legno provenienti dalla bara; 3) frammenti di tessuto umano provenienti dalla salma stessa. I risultati delle misurazioni effettuate non mostrano differenze statisticamente significative; una maggiore differenza può essere rilevata per ciò che concerne l'età del campione di legno, che risulta più antico di circa 50 anni, ma nel complesso le misurazioni sono concordi nel riferire alla metà del XVII secolo l'età della sepoltura. Rilievo Delle Condizioni Patologiche La porzione post-craniale della mummia non mostra caratteri patologici di rilievo. Il cranio è stato studiato sia direttamente che su lastra radiografica e mostra alcune caratteristiche patologiche. Nel suo complesso esso si presenta asimmetrico, infatti presenta un più marcato sviluppo in altezza della porzione parietale destra ed un maggiore sviluppo in larghezza della porzione temporo-occipitale sinistra. Questi caratteri sono apprezzabili su radiogramma dove, ancora più evidente, risulta una maggiore sporgenza della squama dell'osso occipitale tale che, complessivamente, il cranio di questo individuo assume l'aspetto di un cranio conosciuto come "batrocefalico". Inoltre è visibile, sia all'osservazione diretta che su radiogramma, una spiccata asimmetria della mandibola che, sebbene sia stata accentuata per lussazione post-mortale, risulta essere asimmetrica anche nelle sue due porzioni destra e sinistra confrontate fra loro. Una ulteriore osservazione di carattere patologico riguarda i seni frontali che risultano asimmetrici in quanto, a sinistra, è evidente una maggiore ossificazione che potrebbe rappresentare l'espressione di un osteoma o di un processo flogistico cronico di cui il soggetto abbia sofferto in vita. Tale ossificazione, che si accompagna ad una pneumonizzazione del seno frontale di destra, risulta più evidente quando si paragonino i seni frontali fra di loro. Sul corpo della mandibola, inoltre, non sono rilevabili aree di ostelisi riferibili a granulomi apicali, la qual cosa permette di ipotizzare che il soggetto in questione non fosse affetto da carie e pertanto la rilevata edentulia, paragonata alla relativa giovane età del soggetto, potrebbe essere il risultato di una paradontopatia di cui questi abbia sofferto in vita. Un particolare anatomico rilevabile sul cranio, sia direttamente che su radiogramma, è la presenza di alcune ossa wormiane di varia grandezza distribuite lungo la sutura lambdoidea; inoltre si può rilevare la presenza di una sella turcica di aspetto normale. Esami istologici Allo scopo di ottenere informazioni più dettagliate sulla mummia, sono stati prelevati da questa alcuni campioni di tessuto osseo, muscolare e cutaneo. Dopo aver sottoposto i campioni di cute e muscolo a reidratazione in soluzione di Sandison, abbiamo proceduto alla colorazione con ematossilina-eosina. Il campione di osso, proveniente dalla fibula sinistra, è stato in un primo momento decalcificato in soluzione di HCl e successivamente colorato in ematossilina-eosina. I preparati istologici allestiti hanno dimostrato uno stato di conservazione ottimale per l'osso, mentre muscolo e cute si sono rivelati rispettivamente in condizioni discrete e pessime. I preparati istologici allestiti mostrano la presenza di un tessuto osseo trofico, ben conservato, con sistemi osteonici attivi e ben organizzati. In molti osteoni é stata evidenziata la presenza di lacune osteocitiche di forma ovale che rappresentano lo spazio occupato in vita dagli osteociti.
Il tessuto muscolare, preventivamente reidratato, sezionato e quindi colorato con ematossilina-eosina, si presenta in buone condizioni di conservazione. Le sezioni, eseguite longitudinalmente rispetto all'andamento delle fibre, mostrano una struttura fibrillare conservata in maniera eccellente, soprattutto evidente all'osservazione alla birifrangenza, mentre non é stato possibile mettere in evidenza le limitanti cellulari. L'esame istologico del tessuto cutaneo ha dimostrato il pessimo stato di conservazione in cui questo si trova, essendo il tessuto stesso fortemente alterato, di aspetto cribrato, con porosità irregolari e perdita della architettura tissutale; nessuna struttura cutanea o sottocutanea é riconoscibile.
|
THE MUMMY FROM TORRICELLA PELIGNA
by
Prof. Luigi Capasso, The discovery of a mummified body beneath the Church of San Giacomo Apostolo at Torricella Peligna is an event of notable historic and scientific importance, which has provided an opportunity for studying the characteristics of this exhibit, especially in relation to its historic-social, anthropological and medical-scientific settings. Studies carried out have provided certain characteristics concerning the peculiar medical-scientific aspects of this exhibit, in particular the age at death, the sex and height in life, pathological conditions and a determination of the period in which death occurred.
The Mummy of Torricella Peligna is well preserved, but its
discovery and
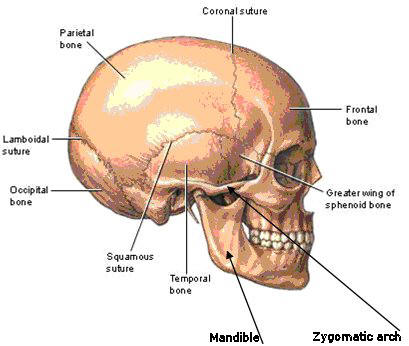
The work of restoration allows for elimination (by means of gaseous disinfectants inserted by complicated manoeuvres) of all destructive agents, from the smallest (bacteria), to the macroscopic (insects). The next phase of conservation is based on creating a “confined microclimate”, that is a glass dome with an internal atmosphere of nitrogen, incompatible with any form of life and isolated from the external environment. Anthropological Relationships Medical-Scientific Features Mummification is an exceptional event, since after death a cadaver usually undergoes decomposition leading to skeletonization. The process of mummification of soft tissues can occur either by natural processes or by artificial manipulation. Artificial mummification was practiced in ancient Egypt and has preserved numerous mummies to the present day, which are still being studied throughout the world. Natural mummification happens in a different manner (saponification[1], mummification in peat, spontaneous mummification), the best known and most common of these is spontaneous mummification. The process of spontaneous mummification takes place under very precise climatic conditions, when the burial environment is very dry and well aired. This leads to a rapid drying out of the soft tissues and thus blocks the action of autolytic[2] tissue enzymes. Another condition capable of influencing spontaneous mummification is the nutritional state of the subject immediately prior to death, mummification occurs more rapidly and with greater ease in subjects who are cachectic[3]. Description of the Exhibit The Mummy under consideration is of a body lying in the supine position, with upper and lower limbs extended, whose overall state of preservation is fairly good although it differs from one part of the body to another. The head is disarticulated from the body and some parts of the face are without skin, also the right ear’s auricle is missing. The trunk is in a good state of preservation and the skin is intact, whereas in some points of the upper and lower limbs, parts the skeleton are visible. Scattered throughout are remains of dead insects which have left evident signs of their demolition work. Anthropological Description The mummified body is of a male subject of adult age. The typical secondary male sexual characteristics are expressed in the head by the general sturdiness of the points of insertion of the muscles of mastication, of the neck and the forehead, from the shape of the mandible which is “stronger” and more square-shaped in the male sex, and also by the greater sturdiness of the various bone segments in general. In our subject these characteristics were evaluated both by direct observation and by X-rays which demonstrate a strong supraciliary[4] arch, the glabella[5], by views of the neck region and of the zygomatic process of the temporal bone[see diagram of skull in Note 9], moreover the body of the mandible is rather large, the chin is very prominent, with an acute profile and a double protruberance of the chin, whilst the gonion[6] shows an extremely prominent coronoid process, the point of insertion of the very powerful masseter[7] muscle. At the level of the pelvis there were external genital organs of the male type and corresponding anthropomorphic characteristics of android pelvic bones, the ileac wings were very narrow and vertical and the ischial aperture (pelvic outlet) was narrow.  As
far as determining the age at death it was noted that the
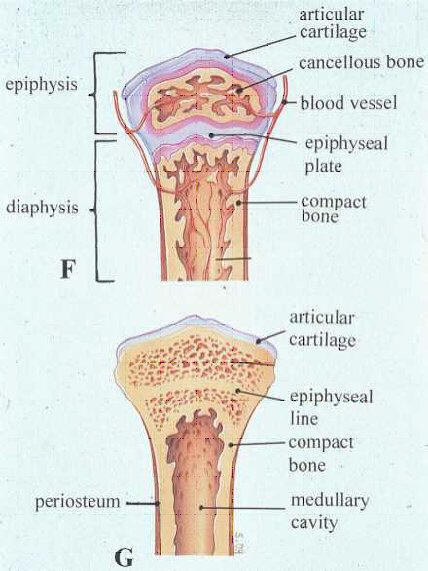
epiphyses[8]
at the As
far as determining the age at death it was noted that the
epiphyses[8]
at the extremeties are ossified[see 8] which places the
subject in an age-band of over 25 years; this was further
confirmed by both direct examination and Xray of the cranial
sutures[9]
and the degree to which they had become fused. These findings
showed that the spheno-occipital suture was partially open, the
lambdoid structure was partially reabsorbed in points 1 and 2 as
indicated by Meindl and Lovejoy[10]
(1985); whilst the coronal and saggital sutures were not easy to
evaluate, Xrays indicated a partial degree of reabsorption.
Moreover there are the results for the Mandible and Maxilla (the
upper jaw) which show a complete absence of teeth, with total
resorption of the alveolar processes[11],
indicating that all the teeth had been lost in life. All these
points lead to the conclusion that age at death was greater than
50 years.
extremeties are ossified[see 8] which places the
subject in an age-band of over 25 years; this was further
confirmed by both direct examination and Xray of the cranial
sutures[9]
and the degree to which they had become fused. These findings
showed that the spheno-occipital suture was partially open, the
lambdoid structure was partially reabsorbed in points 1 and 2 as
indicated by Meindl and Lovejoy[10]
(1985); whilst the coronal and saggital sutures were not easy to
evaluate, Xrays indicated a partial degree of reabsorption.
Moreover there are the results for the Mandible and Maxilla (the
upper jaw) which show a complete absence of teeth, with total
resorption of the alveolar processes[11],
indicating that all the teeth had been lost in life. All these
points lead to the conclusion that age at death was greater than
50 years.The height in life, as measured directly on the mummified body was about 164 centimetres. Investigating the Date of Burial In order to establish when the body was buried, three samples of some organic material from the burial site itself were analysed for chronology using radiocarbon dating methods. The materials examined included: 1) fragments of straw taken from the cadaver’s pillow; 2) fragments of wood from the coffin; 3)
fragments of human tissue taken from the body itself.
Results of measurements carried out do not show any statistically
significant differences; there is a greater difference for the age
of the wood, which proves to be 50 years older, but overall the
measurements agree and place burial in the middle of the 17th
Century. Importance of the Pathological Conditions The bones of the body and limbs of the Mummy, excluding the skull, showed no pathological findings. The skull was studied both directly and on X-ray and showed several pathological features. Overall it shows gross asymmetry, the parietal region is much higher on the right and the left temporal-occipital region is much broader. These features are obvious on X-ray where protrusion of the squama occipitalis[12] is even more evident, giving this individual’s skull the appearance known as Bathrocephaly[13]. There is also a marked asymmetry of the mandible both on inspection and on X-ray which, although accentuated by post-mortem dislocation, shows asymmetry of both the left and the right parts when compared with each other. Other pathological findings were seen at the frontal sinuses which also showed asymmetry, on the left there was much more ossification which could be due to an osteoma[14] or to a chronic inflammatory condition from which the subject suffered in life. This ossification is accompanied by increased air space within the right frontal sinus and becomes even more evident when the frontal sinuses are compared with each other. There are no areas of osteolysis[15] of the body of the mandible, which shows that there were no apical granulomas[16] and that the subject did not suffer from caries and therefore his lack of teeth at this relatively young age was probably due to periodontitis[17] suffered in life. A notable feature of the skull, both on direct examination and on X-ray, is the presence of several Wormian bones[18] of various sizes distributed along the lambdoid suture[see 9]. The sella turcica[19] is normal.
Histological Examination In order to obtain more detailed information about the Mummy, samples of bone, muscle and skin were obtained. Having rehydrated[20] the skin and muscle samples with Sandison’s solution[21], we stained them with Haematoxilin-Eosin[22]. The bone sample, which was taken from the left fibula, was first decalcified in a solution of HCl (hydrochloric acid) and then stained with Haematoxylin-Eosin. The histological preparations showed an excellent state of preservation of the bone tissue, whilst the muscle and skin respectively were fair and poor. The histological preparations showed well preserved well-nourished bone tissue, with a well organised and active osteon[23] system. In many osteons there were oval shaped osteocytic lacunae[24] visible which represent the space occupied in life by osteocytes[25].
The muscle tissue, after rehydration, sectioning and staining with Haematoxylin-Eosin, was in a good state of preservation. Sections, made longitudinally with respect to the muscle fibres, showed an excellently preserved fibrillary[30] structure, especially evident showing as birefringence on polarising microscopy, but it was not possible to show the cell outlines. Histological examination of the skin tissue proved that it was in a very poor state of preservation, the tissue was greatly altered, with a sieve-like appearance, with irregular holes and loss of tissue structure; no cutaneous or subcutaneous structures were recognisable.
|
|
|
| English translation courtesy of Dr. Marion Apley Porreca | |


 relativa
rimozione hanno comportato l'interruzione delle condizioni
ambientali che avevano consentito la mummificazione naturale. Ciò ha
reso necessario realizzare un sistema conservativo suppletivo.
relativa
rimozione hanno comportato l'interruzione delle condizioni
ambientali che avevano consentito la mummificazione naturale. Ciò ha
reso necessario realizzare un sistema conservativo suppletivo.